


|
|
DOI Prefix 10.20431 |
Information
Journal Policies
Study on Knowledge and Practice Regarding Hygienic Conditions among the Residents of Rangeli Municipality of Morang District, Nepal
Ram Bilakshan Sah1, Khadgi A2, Jha N3
2.Junior Resident, School of Public Health and Community Medicine, BPKIHS, Dharan, Nepal
3.Professor & Chief, School of Public Health and Community Medicine, BPKIHS, Dharan, Nepal
Copyright : © 2017 Authors. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Background: Poor hygiene practices play major roles in the increased burden of communicable diseases within developing countries.
Objectives: To assess the knowledge and practice regarding hygienic conditions among residents of Rangeli Municipality of Morang District. To measure the association between sociodemographic characteristics and disease pattern with hygienic practices of the study population.
Methods: A Community based cross-sectional study was conducted from 27th November – 10th December 2016 in Rangeli Municipality where 300 households were taken as subjects. Simple random sampling method was applied. Semi-structured questionnaire was used and face to face interview was conducted. Chi-squaretest was applied to find out the association between sociodemographic characteristics and disease pattern with hygienic practices of the study population.
Results: Majority of participants used soap and water to wash hand before meal (57.3%) and after defection (87%). Most of the study population bathed regularly (59.3%) and cleaned their teeth with brush and toothpaste regularly (92.3%). Almost 99.3% of respondents wear footwear during walking outside. Almost 77.7% of the study population had good hygienic conditions. The study population belongs to above the poverty line and those did not suffer from diarrhea in previous one year had significantly more hygienic practices ((86.1%) and (98.8%) respectively (p< 0.05).
Conclusion: The findings of the study showed that majority of samples had good knowledge and practice regarding hygiene.Overall prevalence of hygienic practices of this study was 77.7%. Higher economic condition and those did not suffer from diarrhea in previous one year was significantly associated with hygienic practices.
Knowledge, Practice, Hygiene, Rangeli Municipality, Morang District,Public Health and Community Medicine
1. Introduction
Hygiene is the basic primary drivers of public health. Access to them ensures personal hygiene and most importantly, human dignity. However, in both rural and urban areas of developing countries, millions of the most vulnerable people lack access to water, making water, sanitation and hygiene (WASH) related infectious diseases the most common causes of illness and death. Nepal is not an exception.[1]
A study conducted by the Global Public–Private Partnership for Hand Washing (PPPHW) which included several sub-Saharan African countries (i.e. Kenya, Senegal, Tanzania, and Uganda) reported that 17% of participants washed their hands with soap after using the toilet, while 45% used only water.9Poorhygienic practices play major roles in the increased burden of communicable disease within these developing countries.[1] Previous hand hygiene studies have indicated that people with proper hand washing practices are less likely to report gastrointestinal and respiratory symptoms.[3], [4]Hand washing with soap has been reported to reduce diarrheal morbidity by 44% and respiratory infections by 23%.[9] Increasing levels of dental caries have been found in some developing countries. Oral health status is an important part of health in general.[6]Traditional methods for mouth cleaning, such as the use of finger or wooden sticks, seem less effective than the use of a toothbrush. Paan chewing represents the most important cause of oral cancer in men and, most notably, in women. Among men, however, 35% of cases are attributable to the combination of smoking and alcohol drinking.[7]Therefore, the present study is undertaken to identify the knowledge and practice regarding hygienic conditions and to find out the association between sociodemographic characteristics and disease pattern with hygienic practices among residents of Rangeli Municipality.
2. Methods
A Community based cross-sectional study was conducted from 27th November – 10th December 2016 in Rangeli Municipality of Morang District of Nepal. Rangeli is located in the eastern geographical region of Nepal. This was a two weeks study to fulfill epidemiological management carried out by students of MBBS 3rd year Batch 2014 of B. P. Koirala Institute of Health Sciences, Dharan, Nepal. This research was based on random selection of the study area Rangeli Municipality.
This study considered 64% of good knowledge about hygienefor sample size estimation.It was calculated as 225.3 by using the formula, sample size (n) = 4 pq/L2 [(n=4 x 64 x 36 / (6.4)2 = 225.3] household as sample based on the prevalence of 64%, 95% confidence level and 10% allowable error. Adding of 15% on final sample for non-response, 226 x 15 / 100= 34, then sample size became 226 + 34 = 260 ≈300.The required sample size is 300 household of ages 18 years and above in Rangeli Municipality of Morang District.11The data was collected from 300 households of ages 18 years and above in Rangeli Municipality. There are 11 wards in Rangeli Municipality. Among 11 wards, 4 wards was randomly selected. The list of households of four selected wards was prepared and equal number of households (75) from each ward was selected on the basis of simple random sampling by lottery method.
Ethical clearance was taken fromUndergraduate Medical Research Protocol Review Board (UM-RPRB) of B P Koirala Institute of Health Sciences, Dharan, Nepal. Written permission was taken from each participants of the study. The participants of both sexes, aged 18 years and above, who were willing to participate in the study, those who gave written consent andthose individuals who were available after three visits were included in the study. Three visits means the selected study subject who was not present at the time of the first visit to the respective place, he or she was followed for three attempts so as to include in the study and in the case of unavailability next study subject was taken.Semi-structured questionnaire and an observational checklist were used for data collectionand face to face interview was taken. The confidentiality and privacy of the study was maintained; name of the individuals or participating group was not disclose after the study.
All interviewed questionnaires were indexed and kept on file. The collected data was entered in Microsoft Excel and converted into SPSS (Statistical Package for Social Science) software package11.5 version for statistical analysis. Data was analysed to find out percentage and proportion, and Chi-square test was used to measure the association between sociodemographic characteristics and disease pattern with hygienic practices of the study population. The confidence level was set at 5% in which probability of occurrence by chance is significant if P< 0.05 with 95% Confidence Interval.
3. Results
Table 1 shows thatmajority of the participants used soap and water to wash hand before meal and after defaecation. Most of the study population bathed regularly and cleaned their teeth with brush and toothpaste regularly. Daily and every alternate day bathed was taken as regular bath, and twice in a week and once a week bathed was taken as irregular bath. Majority of the respondents wear footwear during walking outside.
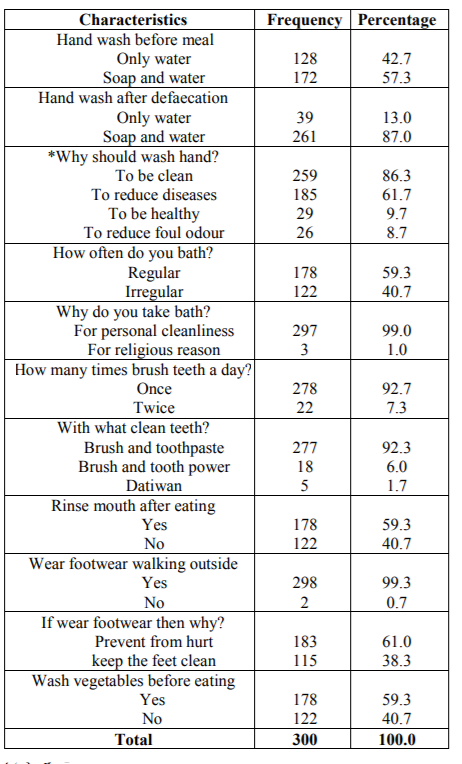
Table 2 shows the majority of the study population had good hygienic conditions. Practice regarding hygiene was accessed by using seven questions: 1.Hand wash before meal, 2. Hand wash after defecation, 3. How often bath, 4. How many times brush teeth a day, 5. Rinse mouth after eating, 6.
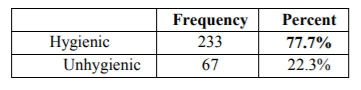
Wear footwear while walking outside, and 7. Wash vegetables before eating. One point was given to each hygienic practice and addition was done with total of maximum seven points for each participants. The points below 3 was considered as unhygienic practices and the points, ≥4 considered as good hygienic practice. Among 300 participants only 233 (77.7%) of the population had good hygienic practices. So the prevalence of hygienic practices of this study was 77.7%.
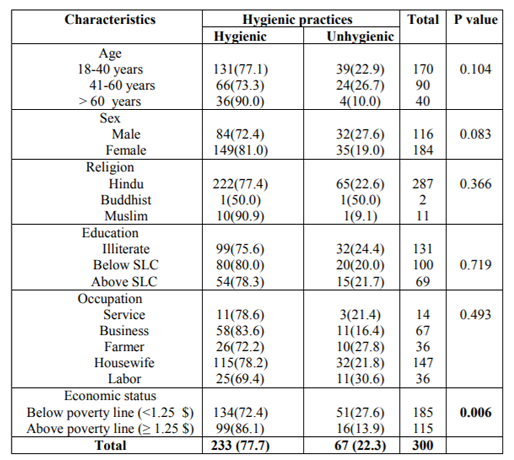
Table 3 shows the study population belongs to above the poverty line had significantly more hygienic practices as compared to people below poverty line (p< 0.05).
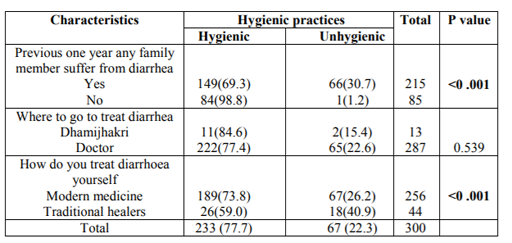
This resultz highlights that those not having diarrhoea in previous one year had better hygienic practices. The study population who treat diarrhea using modern medicine had significantly more hygienic practices as compared to people believe in traditional healers (p < 0.001). (Table 4)
4. Discussion
A large fraction of the world’s illness and death is attributable to communicable diseases.8Sixty-two percent and 31% of all deaths in Africa and Southeast Asia, respectively, are caused by infectious disease.9 This trend is especially notable in developing countries where acute respiratory and intestinal infections are the primary causes of morbidity and mortality.10Poor hygiene practices play major roles in the increased burden of communicable disease within these developing countries.
Our study showed that 77.7% of the study population had good practice on hygiene. A study done in Ethiopia showed 52% had good practice on hygiene.[2]This may be due to the socio-economic condition of Ethiopia being poorer than that of our study population. Likewise, another research done in Kataharivillage of Eastern Nepal found that 64% of the study population had good practice on hygiene which is comparatively poorer than that of our study population.[11]This may be again due to the reason that condition of our study population is better than theirs.
In our study regarding hand wash before meal, majority of participants used soap and water (57.3%). Likewise, in a similar study done in Ethiopia, 99.7% of the study population used soap and water. This may be due to Ethioian cultural beliefs and ceremonial practice of hand washing before eating.[12]Likewise, in a similar study done in India, 38% of the study population practiced hand washing with soap and water before eating meal.[13]
In our study regarding hand wash after defaecation,majority of participants used soap and water (87%). Similar study done in India showed 53% of the study population used soap and water after defaecation.[13]This may be due to the cultural beliefs of hand washing after defaecation. Another study done in Dhankuta showed 95.3% of the study population used soap and water after defaecation.[14]In our study, majority of the participants were having low level of education compared to the study done in Dhankuta.
In this study people reasoned washing of hands to be clean (86.3%), to reduce diseases (61.7%), to be healthy (9.7%) and to reduce foul odour (8.7%). A study conducted by Sah RB et al in Dhankuta Municipality, Nepal in which study people reasoned washing of hands to reduce diseases (71.3%), to be clean (66.3%), to be healthy (39%) and to reduce foul odour (10.7%).14Considerably higher frequency of hand washing in those studies may be due, in part, to the cultural tradition and ceremonial practice of washing hands before meals and after defecation or the desire for clean, fresh hands before eating and after defecation.15,16 Based on the Global Public-Private Partnership for Hand Washing (PPPHW) study conducted in sub-Saharan Africa, motivating factors behind proper hand washing included avoidance of disgust (i.e. avoid dirt and smell of defecation), nurture (i.e. teach children to wash hands so they stay healthy), status (i.e. clean people are more accepted), affiliation (i.e. cleanliness is associated with better socioeconomic status), attraction (i.e. cleaner people are more attractive), comfort (i.e. hands feel and smell fresh), and fear (i.e. avoid the risk of disease).[16]
In our study, majority of study population (59.3%) bathed regularly. Similar study done in Ethiopia showed 58.7% of the study population bathed regularly which was similar to that of our study.2In our study, majority of study population (92.7%) brushed teeth once a day.Similar study done in Ethiopia showed 89.2% of the study population brushed teeth regularly which was slightly lower than our study.
This study shows the majority of the study population (77.7%) had good hygienic practices. Among them 84/233 (36.1%) males and 149/233 (63.9%) females had good hygiene practices.A study conducted by Sah RB et al in Dhankuta Municipality, Nepalshowed 61.6% male and 92%female have proper practice of hygienewhich was higher than our study.14But a study conducted by Lopez-Quintero C et al in Bogota, Colombia showed 52% of respondents had proper practice of hygiene which was lower than our study.[17]
Another reason that can influence hygiene practice among households is the low level of literacy. In our study the household’s literacy rate was higher (78.3%) than a study conducted by Nematian J et al in Tehran (39.7%).18Illiterate or uneducated households may be less knowledgeable about teaching their family member about proper hygiene practices, subsequently leading to increased rates of infection and disease amongst their family member.[18]
Our study showed the association between socio-economic status and hygienic practices of the study population. Participants belong to above the poverty line had significantly more hygienic practices as compared to those below poverty line (p< 0.05). Similarly study done in India also showed significant association of economic status with the hygienic practices.13The individuals belong to the above poverty line had better quality of life than those of below poverty line.
Several limitations must be considered when interpreting our results. First, participants self-reported behaviors may have resulted in over-reporting of proper hygiene practices. We attempted to mitigate this bias by including objective measures of resident’s personal hygiene characteristics. Data from observations were generally consistent with participant’s self-reported practices. Second, the cross-sectionalstudy design makes determining causality impossible.
5. Conclusion
The findings of the study showed that majority of samples had good knowledge and practice regarding hygiene.Majority of the participants used soap and water to wash hand before meal and after defection. Most of the respondents think hand washing is to clean the body and to reduce diseases. Overall prevalence of hygienic practices of this study was 77.7%.Most of the study population bathed regularly, cleaned their teeth regularly and wear sandals or shoes during walking outside.Higher economic condition andthose did not suffer from diarrhea in previous one year was significantly associated with hygienic practices.
Acknowledgement
We would like to thank to School of Public Health and Community Medicine for approval of our research work. We express our sincere thanks to MBBS (2014 Batch) students who helped us during study period.
References
- Water aid report, access to water, sanitation, and hygiene for people living with HIV/AIDS; a cross sectional study in Nepal, 2010.
- Vivas AP, Gelaye B, Abost N, Kumie A, Berhane Y, Williams MA. Knowledge, attitudes and practices (KAP) of hygiene among school children in Angolela, Ethiopia. J prev med hyg 2010; 51: 73-79.
- GoN, sanitation and hygiene master plan, 2011. Available at: http:// washins chools mapping.com/wengine/wp-content/uploads/2015/10/Nepal-Government-Sanitation-and-Hygiene-Master-Plan.pdf. (Accessed on 30 January 2017)
- WHO, official list of MDG goals, 2015. Available at: www.Womenandchildrenfirst.org.uk. (Accessed on 30 January 2017)
- Ejemot RI, Ehiri JE, Meremikwu MM, Critchley JA. Hand washing for preventing diarrhoea. Cochrane Database Syst Rev 2008; 23 (1). CD004265.
- World Resources Institute, United Nations Development Programme, the World Bank. World Resources 1996-97 - The Urban Environment, Oxford University Press, Oxford, 1996.
- Burt BA. Trends in caries prevalence in North American children. Int Dent J 2014; 44: 403-413.
- World Health Organization. Better health for poor children, 2010. Available at: http:// www.who.int/child_ adolescent_health/documents/a91061/ en/index.html. (Accessed on 30 January 2017)
- Curtis VA, Danquah LO, Aunger RV. Planned, motivated and habitual hygiene behaviour: an eleven country review. HealthEduc Res 2009;4:655-73.
- World Health Organization. Hand-washing could save the lives of millions of children, 2010. Available at: http://www.scielosp.org/scielo.php?lng=en. (Accessed on 30 January 2017)
- Karn RR, Bhandari B, Jha N. A study on personal hygiene and sanitary practices in a rural village ofmornag district of Nepal. Journal of Nobel Medical College2011;1 (2): 39-44.
- Intercultural Communication Specialists Ethiopia: Language, Culture, Customsand Etiquette,2012. Available at: http://www.Kwintessential. co.uk/ resources/ globaleti quette/ethiopia.html. (Accessed on 30 January 2017)
- Reshma, Mamatha, S. Pai & Manjula. A Descriptive Study to Assess the Knowledge and Practice Regarding Water, Sanitation and Hygiene among Women in Selected Villages of Udupi District1. NUJHS2010; 6 (1): 2249-7110.
- Sah RB, Bhattarai S, Baral DD, Pokharel PK. Knowledge and Practice towards hygiene and sanitation amongst residents of Dhankuta Municipality. Health Renaissance2014; 12 (1): 44-48.
- Intercultural Communication Specialists Ethiopia: Language, Culture, Customs and Etiquette 2012. Available at: http://www. Kwintessential. co.uk/ resources/global etiquette/ethiopia.html. (Accessed on 30 January 2017)
- Scott B, Curtis C, Rabie T. Health in our hands but not in our heads: understandinghygiene motivation in Ghana. Health Policy and Planning 2007; 22: 225-233.
- Lopez-Quintero C, Freeman P, Neumark Y. Hand washing among school childrenin Bogota, Colombia. Am J Public Health 2009; 99:94-101.
- Nematian J, Nematian E, Gholamrezanezhad A, Asgari AA. Prevalence of intestinal parasitic infections and their relation with socio-economic factors and hygienic habits in Tehran primary school students. Acta Trop 2004; 92:179–86.